The Knee That Never Fully Healed — How Shockwave Therapy Addresses Chronic Joint Pain
You remember exactly when it happened. A misstep on the court. An awkward landing coming off a bike. A moment during a round of golf where something didn't feel right. Or maybe there wasn't a single moment at all — just a gradual accumulation of miles, matches, and mornings until the knee started talking back.
Either way, the story tends to follow the same arc. You rested it. You did the physical therapy. You got the injection. It got better — not all the way, but enough to get back to doing what you love. And then it plateaued. Months later, sometimes years later, the knee still isn't right. Recovery after activity takes longer than it should. There's a stiffness in the morning that wasn't there before. A dull ache that flares up when you push harder than usual.
This is one of the most common — and most undertreated — situations facing active adults in their 40s, 50s, and 60s. And it's precisely the kind of problem shockwave therapy is designed to address.
Why Chronic Knee Pain Is Different From Acute Knee Pain
The distinction matters because the treatment approach is different.
Acute knee pain — the kind that follows a fresh injury — triggers an immediate biological response. The body floods the area with inflammatory cells, increases blood flow, and initiates the repair cascade. This process is uncomfortable, but it's purposeful. Given time and appropriate care, many acute injuries resolve.
Chronic knee pain is a different animal. In these cases, the initial repair response has wound down — but the underlying tissue damage hasn't fully resolved. The body has, in a sense, stopped prioritizing the area. The tissue quality is compromised. The tendon, cartilage, or surrounding soft tissue is structurally different than it was before the injury. And because there's no active inflammatory signal driving repair, conventional anti-inflammatory treatments — rest, ice, cortisone — have limited impact on the root issue.
What's needed isn't suppression of inflammation. What's needed is a renewed repair response.

What Shockwave Therapy Does for the Knee
Shockwave therapy delivers focused acoustic pressure waves into the soft tissue, tendons, and structures surrounding the knee joint. This mechanical stimulus triggers a series of biological responses that conventional treatments don't produce.
Specifically, in the context of chronic knee pain, shockwave therapy addresses four key mechanisms:
Restimulates the repair response. The acoustic energy signals to the tissue that repair resources are needed. Blood flow increases. Fibroblast activity — the cellular mechanism behind collagen production — is elevated. The area becomes biologically active again in a way it hasn't been since the acute phase of the original injury.
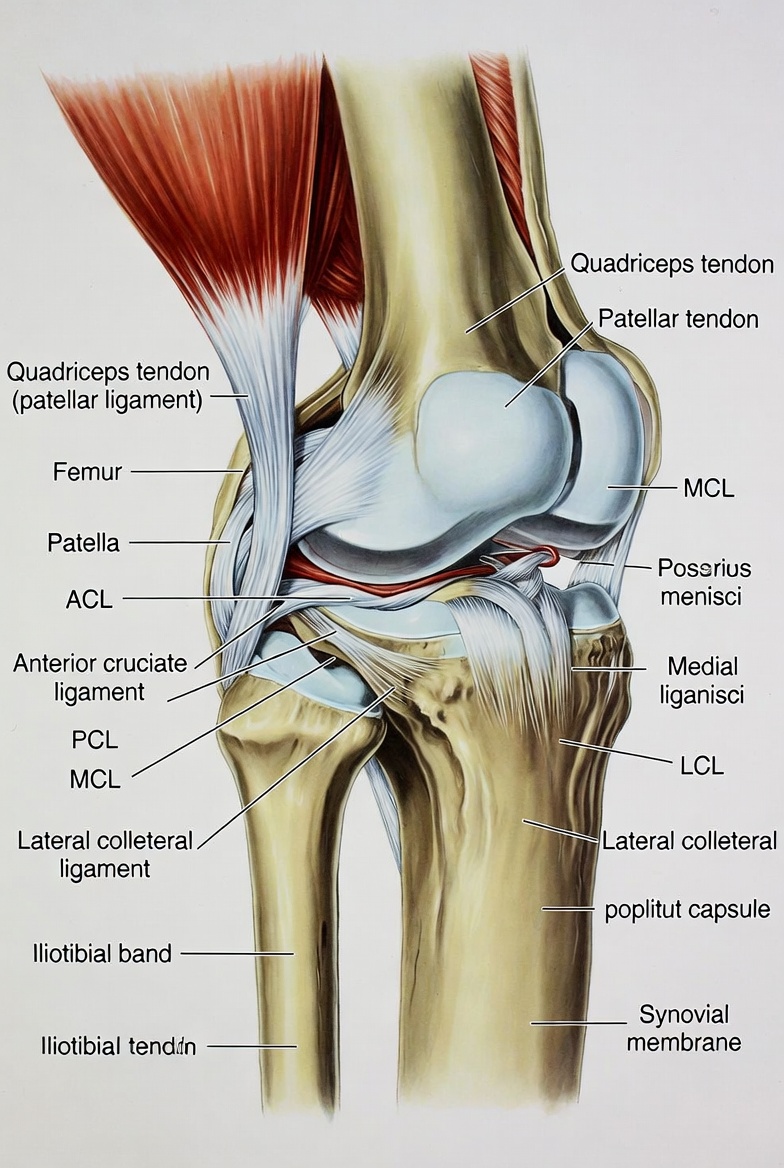
Addresses tendon degeneration. Many cases of chronic knee pain involve the patellar tendon — the tendon connecting the kneecap to the shinbone. When this tendon is repeatedly stressed without adequate recovery, the tissue quality degrades. Shockwave therapy has a well-documented track record for patellar tendinopathy specifically.
Disrupts calcific deposits. In some patients, calcium has accumulated around the joint or in the surrounding soft tissue. Shockwave therapy breaks up these deposits, which can restore mobility and reduce the mechanical irritation they cause.
Modulates pain signaling. Beyond the structural repair mechanisms, shockwave therapy also influences the nerve fibers responsible for transmitting pain signals from the knee. Many patients notice a meaningful reduction in baseline discomfort within the first few sessions — before the full tissue remodeling effect has taken hold.
Who This Approach Is Best Suited For
Not every knee condition is a shockwave candidate, and Harper MD doesn't position it as one. But for a specific profile of active adult, it's one of the most effective tools available.
You may be a strong candidate if:
•Your knee pain has persisted for three months or more without full resolution
•You've completed a course of physical therapy with partial but not complete improvement
•You've had one or more cortisone injections that provided temporary relief but didn't hold
•Your imaging shows soft tissue or tendon involvement rather than severe structural deterioration
•You've been told surgery is a possibility — but you're not ready to commit to that path
•Your knee pain is affecting your ability to train, compete, or stay active at the level that matters to you
If advanced joint degeneration or structural damage is severe enough that the tissue environment can no longer support meaningful repair, shockwave therapy alone may not be sufficient. An honest evaluation — one that looks at your history, your imaging, and your goals — will determine whether this is the right next step.
Shockwave vs. The Treatments You've Already Tried
Most active adults who arrive at shockwave therapy have already been through the conventional treatment sequence. Understanding where shockwave fits relative to those options helps clarify why it can succeed where others have plateaued.
vs. Cortisone injections. Cortisone reduces inflammation effectively in the short term. But it doesn't rebuild tissue — and repeated injections can degrade tendon integrity over time. For chronic tendon conditions, the evidence increasingly favors shockwave as a more durable long-term option because it addresses the tissue environment rather than suppressing the inflammatory signal.
vs. Physical therapy. Physical therapy is valuable, and it often works alongside shockwave therapy rather than instead of it. Where PT addresses strength, mobility, and movement mechanics, shockwave addresses the tissue-level environment that determines whether those gains hold. For patients where PT has plateaued, shockwave can restart the process.
vs. Waiting it out. Chronic knee conditions tend not to resolve on their own once the acute phase has passed. Without an intervention that actively restimulates repair, the tissue environment remains compromised — and the issue typically compounds with continued activity. Earlier intervention produces more durable results than delayed action.
vs. Surgery. Surgery is appropriate when structural damage is severe enough that non-invasive approaches can't address the underlying issue. For many of the conditions where shockwave is indicated, surgery isn't the first recommendation — it's a last resort. Shockwave therapy is most valuable in the space between 'it's not getting better on its own' and 'surgery is necessary.'

What to Expect From the Process
A shockwave therapy protocol for chronic knee pain typically involves three to six sessions, spaced approximately one week apart. Sessions run 15 to 30 minutes. There is no anesthesia required, no recovery period, and no restriction on normal daily activity following treatment.
During each session, a conductive gel is applied to the knee area and the shockwave device is placed against the skin over the targeted tissue. You will feel pressure — and in areas of active tissue damage, some discomfort. That discomfort is expected and is part of how the treatment works. It typically fades quickly after the session ends.
Mild soreness in the knee for 24 to 48 hours following treatment is common. This reflects the tissue response that has been initiated — not damage. Most patients find it manageable and return to their normal schedule the same day.
Results vary by individual, condition severity, and chronicity. Some patients notice improvement after two or three sessions. Others see the most significant change in the weeks following the completion of the full protocol, as the tissue remodeling process continues.
How Shockwave Fits Into a Broader Joint Restoration Plan
For many patients, shockwave therapy is most effective as part of a broader joint restoration approach rather than a standalone treatment. At Harper MD, it often works alongside cellular regenerative therapy, peptide therapy, and a structured plan that accounts for the whole picture — not just the knee in isolation.
The active adults who respond best to this kind of approach tend to share one characteristic: they address the issue before it compounds. The knee that's been limiting training for six months is a better candidate than the knee that's been ignored for a decade. The tissue environment is more responsive. The repair capacity is greater. And the path back to full function is more direct.
If your knee has been limiting you — and you've been waiting to see if it resolves on its own — it's worth understanding whether shockwave therapy is appropriate for your situation. An evaluation at Harper MD starts with a thorough conversation about your history, your activity level, and your goals. No generic protocols. No assumptions. A clear-eyed assessment of what's happening and what the options are.

Frequently Asked Questions
How long before I notice results? Some patients notice improvement within the first two to three sessions. For others, the most meaningful change occurs in the two to four weeks following the completion of the full protocol, as the tissue remodeling process continues after treatment ends. Individual response varies based on the condition, its chronicity, and the degree of tissue involvement.
Can shockwave therapy help if I have arthritis in my knee? It depends on the severity and the nature of the damage. Shockwave therapy is most effective for soft tissue and tendon involvement. In cases of moderate joint degeneration, it can still be a useful part of a broader joint restoration plan. In cases of severe structural deterioration, the approach may need to be different. An evaluation will clarify which applies to your situation.
Is this the same as ultrasound therapy? No. Ultrasound therapy uses sound waves at a much lower energy level, primarily to warm tissue. Shockwave therapy uses high-energy acoustic pressure waves specifically calibrated to trigger a biological repair response. They are different technologies with different mechanisms and different clinical applications.
Do I need to stop exercising during treatment? Not necessarily. Your provider will give you specific guidance based on your condition and activity level. In most cases, moderate activity is maintained throughout the protocol. High-intensity loading of the treated area may be temporarily modified during the treatment course.
Harper MD | 17150 Royal Palm Blvd #3, Weston, FL 33326 | (954) 338-1111 | harpermd.com
This content is for educational purposes only and does not constitute medical advice. Individual results vary. Consult a qualified healthcare provider to determine whether shockwave therapy is appropriate for your specific situation.
